
Have you recently been scrolling on social media while “sittervising” your kids at The Gathering Place in Tulsa and been introduced to the very opinionated world of online pelvic floor physical therapy? You may have seen bold statements like “never do kegals!” or “stop doing this if you have a diastasis!” or “do this one exercise to help with prolapse!” Online messages can be tricky to decode because they are vying for your attention with very bold claims in a one-size fits all type approach which most people do not fit into. Rehab should be nuanced and take a more holistic approach that incorporates all relevant factors into consideration. A one-size fits may not help at all, or help temporarily but never get to the source of the issue. Today we are decoding and myth-busting some bold claims that you may have seen online or heard from a friend.
Myth 1: kegals help all pelvic floor conditions!
False! If you suspect that you have a pelvic floor condition, Dr. Google is sure to recommend kegals for any and all dysfunctions related to that region of your body. However, they may not be helpful for everyone. Those who have pelvic and low back pain may have pelvic floor muscles that are already working too hard and need to relax instead of contract (aka a kegal). By doing more kegals you may be exacerbating the problem instead of helping it.
Myth 2: nobody should do kegals, ever!
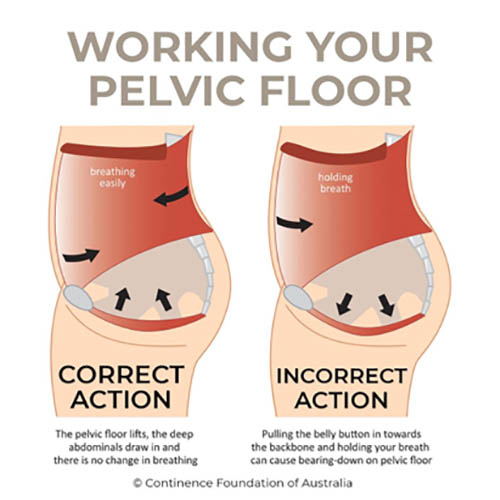
False! If you have a pelvic floor that is unable to produce a strong contraction or unable to hold that contraction, kegals may be an appropriate intervention for you. A kegal is an isolated pelvic floor muscle contraction therefore by contracting those muscles, you will help to make them stronger. Although kegals may be an appropriate intervention for some, it should never be the only intervention as the pelvic floor works as a team with the deep core muscles (transverse abdominus), the breathing muscle (diaphragm) and is influenced by hip and back functioning too. If you are doing kegals, make sure that you are performing them correctly by squeezing up and in (think about picking up a marble with your vagina) and not bearing down while holding your breath.
Myth 3: incontinence is inevitable after I have had a baby!
False! Although there is a significant load and strained placed on the pelvic floor throughout pregnancy and there can be injury to the pelvic floor and pelvic nerves with delivery, these structures have the ability to heal and be retrained postpartum to ensure that you can jump on the trampoline with your little ones without leaking everywhere. With the right guidance and support in your postpartum journey, you are not doomed to a life of incontinence.

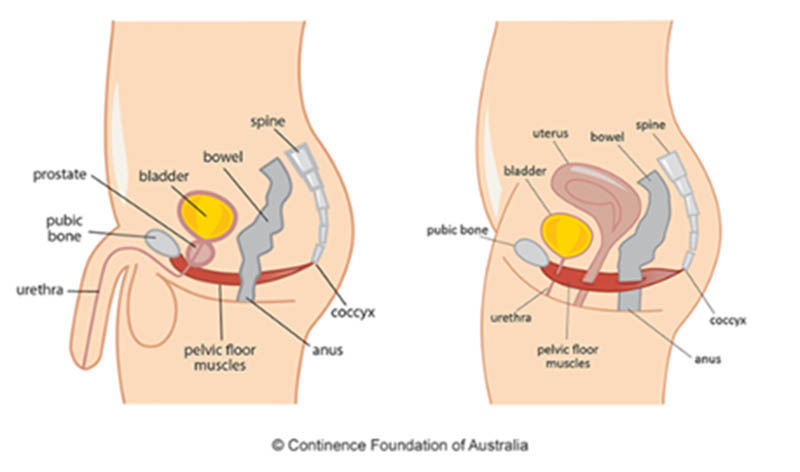
Myth 4: only women have pelvic floors and can have “pelvic floor dysfunction”!
False! Men also have pelvic floors and therefore can also experience pelvic floor dysfunction. Common dysfunctions of the pelvic floor that men face include erectile dysfunction, pelvic pain, increased muscle tension of the pelvic floor, pudendal neuralgia, urinary dysfunction including difficulty starting stream, incontinence and dribbling after urination. The male pelvic floor gets less attention because due to the structure of the muscles and fascia of the pelvic floor as well as the layout of the urinary system, men are less likely to experience incontinence. Cis males also do not experience pregnancy or birthing, which can lead to some pelvic floor dysfunctions, and are therefore less likely to be exposed to the location and function of the pelvic floor like females may be.
If you found this informative, lookout for Part 2 of the pelvic floor myth-busting series or visit us in Tulsa for an individualized evaluation and plan of care suited for your particular needs.